- Subject Code : ENGR9741
- University : Flinders University My Assignment Services is not sponsored or endorsed by this college or university.
- Subject Name : Engineering
Contents
1 Introduction
2 Background Information of the Instrument
2.1 Overview of the Instrument
2.2 History
2.3 Measures and Process of Measurements
2.4 Range of Values and Limits
3 Physiological and Medical Correlates
3.1 Physiological Correlates with the Measurement
3.2 Medical Conditions Implied by the Measurement
4 Use of the Instrument
5 Conclusion
6 References
Introduction
The report presents detailed discussions and information related to the medical device, pneumotachometer, which is used for evaluating the breathing and respiratory characteristics of people, in medical usage and applications. A pneumotachometer helps in measuring the direct airflow in the lungs of a person/patient by measuring the instantaneous flow of gases based on the exhaled flow of air (Macia, 2006).
The report thus focuses on providing basic information of the device along with physiological information and background. First part of the report provides basic information of the device wherein it provides information on its history, its measurements, the way it is utilised and processing of the measures obtained. The report further evaluates the physiological and medical correlates of the device wherein the physiological analysis is related to the analysis of functions and functionalities as associated with humans. These discussions have thus helped in understanding the medical correlates associated with the measurement and the way it is utilised in different medical settings.
Background Information of The Instrument
Overview of The Instrument
A pneumotachometer as explained by Rosengarten et al. (2003), refer to the devices that are flow resistive in nature that allows the flow of gas via a specific tube that contains specific element which is flow resistant in nature wherein the element that is used for flow resistant can be either entire bundle of small capillaries or a fine-mesh screen. The pressure differences that tend to arise during the flow of the gas through this fine mesh helps in measuring the rate at which the gas is flowing (Rosengarten et al., 2003). It is considered to be a spirometer that allows the measurement of the overall air volume that is inspired as well as expired via the lungs of humans.
While there are a large number of spirometers that are present in the market and are being used for breathing measurement purposes, Dominelli and Sheel (2012) establish that a pneumotachometer is considered to be extremely beneficial because it allows the patient under review to be able to breathe fresh air while the experiment is being carried out. There are in fact several different types of pneumotachometer that are used for medical applications that include lilly, fleisch, turbine, venture and ultrasonic (Dominelli & Sheel, 2012).
History
The history of the device can be understood better with the help of the history of spirometers that are in general used for breathing and respiratory measurements. The first spirometer was indeed developed in the nineteenth century by John Hutchinson who developed over 4000 spirometers (O'Reilly, 2016). The rationale or the logic that was used by him for development of a spirometer was based that the longevity of a person can be measured based on the volume of air that is exhaled via an inflated lung (O'Reilly, 2016).
After the first application of a spirometer in 1958, the first pneumotach system was developed in the year 1963 that was successful in measuring the pressure-volume curves (Macfarlane, 2017). There were several different types of pneumotachometer that were then being developed by the 90s that made use of different outer material and internal element (Macfarlane, 2017). The device in the twenty first century has been made highly sophisticated with advanced technologies and features.
Measures and Process of Measurements
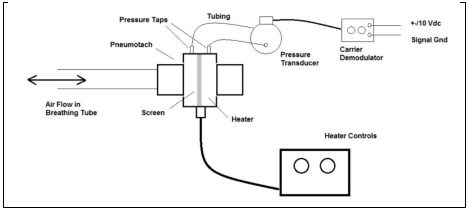
Figure 1: Pneumotachometer Device
Pneumotachometer is primarily used for measuring the volume as well as the speed at which a person is able to breathe air. As shown in figure (1), the device consists of a pneumotach that is inserted within the airflow such that it connects to the patient via an air-tube without causing any restrictions in his/her ability to breathe (Balleza et al., 2007). Movement of air within the device results into change in pressure across the screen. As the pressure changes, pneumotach screen records analog signals that help in measuring volume of air flow (Balleza et al., 2007). In fact, there are different ways in which the flow of air can be measured, thus leading to the following types of pneumotachometers:
-
Pressure Differential: This type of pneumotachometer is a special fleisch type device that makes of the use of pressure differential created during breathing for measurement.
-
Thermistor: The pneumotachometer device makes use of changes in temperature for measurement (Shelledy & Peters, 2014).
-
Turbinometer: Turbinometers do not use pressure or temperature but rather makes use of the rotations of fans that are included within the system to assess speed as well as volume of rotation (Shelledy & Peters, 2014)
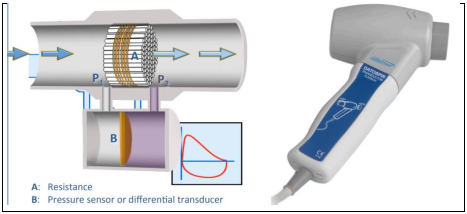
Figure 2: Fleisch Pneumotachometer
The most commonly used pneumotachometer is the fleisch pneumotachometer that is primarily based on the overall pressure of the air that flows through the system before and even after passing through the given resistance (Snepvangers et al., 2003). Measurement of this device can be explained based on the image given in figure 2. A is the resistance that is kept proportional to the overall air flow passing through the sensor used to measure the pressure (part B). Thus, the pressure P1 as created before the resistance and P2 as created after the resistance are measures, to assess the volume of air flow (Schena et al., 2012).
This type of pneumotachometer is considered to be the most efficient because it is extremely simple to use and is considered to be safe to use on people because of lack of any electronic parts or devices that come close to the patients (Schena et al., 2012). Cooper (2020) stated that this device aligns with quality requirements as defined by the ISO 26782:2009 standard and can be easily recalibrated for higher accuracy.
Range of Values and Limits
The device is used for measuring the flow of air from 0 to 14 l/s wherein the precision of -3% to 3% is considered. As explained by Snepvangers et al. (2003), the oxygen concentration in the flow of air is a key measure and the level of oxygen flow is processed in order to make the measurement wherein the flow can be anywhere between 0% and 100%. The device is usually calibrated and scaled based on the characteristics of the patient for whom the device is being used based on their age, gender, physical characteristics etc. (Snepvangers et al., 2003). Thus, this is how the device of pneumotachometer is utilised for the purpose of measuring respiratory characteristics of the patients. Further analyses focus on evaluating key physiological and medical correlates of the device.
Physiological and Medical Correlates
Physiological correlates are primarily used to carry out an analysis of the way physiological measures underlying a given concept can be related and associated with the behavioural measures (Cauffman et al 2005). The correlates help in establishing the existence of a casual relation between the physiological and behavioural measures and not necessarily the cause that is responsible for it (Cauffman et al., 2005). Further discussions focus on evaluating the physiological correlates surrounding the measurements by a pneumotachometer followed by evaluation of the different medical conditions that are implied based on the measurements provided by the device.
Physiological Correlates with The Measurement
The physiological correlates of the measurements carried out by a pneumotachometer relate to the various correlates that can be associated with air flow and breathing of people in general. As the device is used for measuring the airflow in people at the time of normal breathing the natural air, it helps in analysing the breathing patterns and normality of human bodies (Didierlaurent et al., 2013). It helps in measuring respiration as observed in humans based on the regular breathing of natural air by them. The device focuses on two important physiological measurements, i.e. the volume and amount of air that comes out from the nostrils of people at the time of breathing. In addition, it is also used for the measurement of airflow as observed during speech (Didierlaurent et al., 2013)
The physiological characteristics and relevance of respiration have been explained by Birn(2012), who establishes that respiration is usually considered to be the oscillator that helps in facilitating the regulation of different processes that change in response to the different environmental factors and demands. There are specific pacemaker neurons in human bodies that tend to influence and affect the rhythm of respiration, thus affecting the volume and speed of airflow from the lungs. The use of the device thus not only helps in assessing the volume and speed associated with flow of air during respiration, but also helps in measuring the way the flow changes due to the presence of one or other forms of resistance (Saboisky et al., 2007)
Primary sensing element in device is thus said to be the changes observed in the flow of air, which in turn helps in calculating different elements of the pulmonary functions of human bodies. Breathing frequency as highlighted by Sierra et al. (2006), under normal circumstances is around 15 respiratory cycles every minute and thus the use of the pneumotachometer helps in assessing if the respiratory cycle is normal or not. As the activities being carried out by the human body tend to change, not only does the frequency changes, but also the tidal volume, i.e. the volume of air that is drawn in and also exhaled by the lungs, tend to change.
Hence the physiological correlates underlying the device are primarily useful for measuring different aspects and measures of respiration and related activities of human bodies. The measurements that are obtained under ambient conditions are utilised further to carry out an assessment of the conditions that are present in the lungs. Some of the key medical conditions that can be implied by the measurements obtained from the device are being analysed further.
Medical Conditions Implied by The Measurement
The device, pneumotachometer, is primarily used to imply medical conditions associated with breathing of people in general. One of the common medical conditions implied by the measurement by the device is that of asthma. Asthma is a lung disease, which suggests obstruction of the airflow in the lungs (Morgan et al., 2005). According to the analyses by Morgan et al. (2005), asthma is a common respiratory medical condition that usually remains undiagnosed and is analysed with the help of spirometry that is largely based on the use of pneumotachometer. In addition to asthma, another medical condition that remains undiagnosed and can be implied by the measurements through pneumotachometer is chronic obstructive pulmonary disease (COPD).
COPD refers to the medical condition wherein the flow of air in the lung gets obstructed, thus resulting into long-term breathing issues (Balleza et al., 2010). The effectiveness of using a pneumotachometer for implying COPD has been highlighted by academics (Balleza et al., 2010: Feshchenko et al., 2014; Ordaz et al., 2009). Madueno et al. (2009) carried out an experimental study of patients in Spain. The authors have highlighted the use of a pneumotachometer that was used to measure the forced vital capacity ratio (FCV), which was used to assess the lung capacity and functioning of the individuals. Hence, the device is used for identifying and implying the medical conditions of asthma and COPD.
In addition to these commonly observed lung diseases, the device also implies other medical conditions such as chronic bronchitis, emphysema and pulmonary fibrosis. These medical conditions are associated with the overall capacity and capability of human lungs to be able to facilitate or block the flow of air through them, which, in turn, determines if the individuals have a breathing issue or not (Usemann et al., 2017). The use of the device can be explained based on the discussions regarding spirometry, wherein academics (Madueno et al., 2009; USemann et al., 2017) explain that spirometry is extremely useful in medical world because it allows the medical practitioners to identify the activity restrictions and limits that must be imposed on each individual based on their respiratory and breathing characteristics.
In fact, it is also useful for measuring and deducing the effectiveness of different medicines that are used by medical practitioners to affect and influence the level of breathing. It can be thus deduced that the use of the device of pneumotachometer is beneficial in identifying any underlying medical condition associated with breathing wherein breathing issues are caused due to the amount of air flow and obstruction caused due to it.
Use of The Instrument
Pneumotachometer is a diagnosis device that is adopted for the diagnosis and identification of medical conditions and issues related to breathing. The device does not facilitate any treatment or correction that can improve the breathing conditions and/or flow of air in and out of the lungs of patients (de Sa et al., 2016). The most common application of the device is by the pulmonologists, the physicians who specialise in diagnosing and treating breathing related disorders. These physicians use the device in regular lab or clinical setting such that they are able to identify the respiratory diseases or challenges that their patients are facing. Pulmonary function testing is the key application by the physicians (de Sa et al., 2013).
However, the use of the device is not restricted to this. According to the discussions by Kalicka et al. (2007), spirometry and its related devices are commonly used before and after surgeries. Use of pneumotachometer before a surgery helps the doctors in identifying if there are any underlying breathing or respiratory issues that are being faced by the patient such that they can determine and identify whether the surgery is safe or not and whether they need to undertake additional precautions during the surgery. In fact, it has been found that the patients are also given pneumotachometer after a surgery such that they can measure and monitor their own breathing patterns to be able to identify any irregularities that can be useful for diagnosing the problems early (Kalicka et al., 2007). The progress of treatment as observed for a condition and also the impact of medicines can be diagnosed and identified with the help of the device.
These discussions suggest that a pneumotachometer is primarily a device used for the purpose of diagnosis. But its application for treatment purposes also does exist. One of the key roles of the device is in measuring the effectiveness of treatment that is being used by any medical specialist. But interestingly, academics like Heinzer et al. (2005) and McGinley et al. (2007) have also established the use and role of the device in treating sleep apnea. McGinley et al. (2007) explain that respiratory conditions are the key underlying causes of sleep apnea and thus the use of a pneumotachometer helps in identifying and implementing suitable treatment for it. These discussions thus suggest that the application of the device of pneumotachometer is multi-fold and can be utilised in different scenarios by different medical experts.
Conclusion
The report has helped in evaluating and analysing the application and physiology of the medical device of pneumotachometer. The device is adopted and utilised for the measuring air flow volume and speed in and out of lungs of humans. The device helps in assessing the respiratory aspects and characteristics of people, which thus helps in establishing and measuring different issues related to breathing and respiration such as asthma and COPD. Main application of the device is for diagnosis of medical conditions, but it does help in facilitating treatment of some conditions as well.
References
Balleza, M., Fornos, J., Calaf, N., Feixas, T., Gonzalez, M., Anton, D., ...&Casan, P. (2007). Monitoring of breathing pattern at rest by electrical impedance tomography. Archivos de Bronconeumología ((English Edition)), 43(6), 300-303.
Balleza, M., Anton, D., Casan, P., &Riu, P. (2010). Tidal Volume (TV) post-process obtained with Electrical Impedance Tomography on a group of chronic obstructive pulmonary disease (COPD) patients. Use of adjust equations. In Journal of Physics: Conference Series (Vol. 224, No. 1, p. 012030). IOP Publishing.
Birn, R. M. (2012). The role of physiological noise in resting-state functional connectivity. Neuroimage, 62(2), 864-870.
Cauffman, E., Steinberg, L., &Piquero, A. R. (2005). Psychological, neuropsychological and physiological correlates of serious antisocial behavior in adolescence: The role of self‐control. Criminology, 43(1), 133-176.
Cooper, B. G. (2020). Basic equipment and measurement techniques. Cotes’ Lung Function, 91-116.
de Sa, P. M., Castro, H. A., Lopes, A. J., & de Melo, P. L. (2016). Early diagnosis of respiratory abnormalities in asbestos-exposed workers by the forced oscillation technique. PloS One, 11(9).
de Sa, P. M., Lopes, A. J., Jansen, J. M., & de Melo, P. L. (2013). Oscillation mechanics of the respiratory system in never-smoking patients with silicosis: pathophysiological study and evaluation of diagnostic accuracy. Clinics, 68(5), 644-651.
Didierlaurent, D., Ribes, S., Caselles, O., Jaudet, C., Cazalet, J. M., Batatia, H., &Courbon, F. (2013). A new respiratory gating device to improve 4D PET/CT. Medical Physics, 40(3), 032501.
Dominelli, P. B., &Sheel, A. W. (2012). Experimental approaches to the study of the mechanics of breathing during exercise. Respiratory Physiology & Neurobiology, 180(2-3), 147-161.
Feshchenko, Y., Iashyna, L., &Opimakh, S. (2014). The use of capnometry for alveolar ventilation assessment in COPD patients. European Respiratory Journal, 44(Suppl 58), P2128.
Heinzer, R. C., Stanchina, M. L., Malhotra, A., Fogel, R. B., Patel, S. R., Jordan, A. S., ... & White, D. P. (2005). Lung volume and continuous positive airway pressure requirements in obstructive sleep apnea. American Journal of Respiratory and Critical Care Medicine, 172(1), 114-117.
Kalicka, R., Slominski, W., &Kuziemski, K. (2007, September). Modelling of spirometry. Diagnostic usefulness of model parameters. In EUROCON 2007-The International Conference on" Computer as a Tool" (pp. 2137-2143). IEEE.
Macfarlane, D. J. (2017). Open-circuit respirometry: a historical review of portable gas analysis systems. European Journal of Applied Physiology, 117(12), 2369-2386.
Macia, N. F. (2006). Pneumotachometers. In: Webster, J.G. (ed.) Encyclopedia of Medical Devices and Instrumentation. 2nd ed. New York: Wiley, 2006, 367-379
Madueño, A., Martín, A., Péculo, J. A., Antón, E., Paravisini, A., & León, A. (2009). Usefulness of inspiratory capacity measurement in COPD patients in the primary care setting. International Journal of General Medicine, 2, 219.
McGinley, B. M., Patil, S. P., Kirkness, J. P., Smith, P. L., Schwartz, A. R., & Schneider, H. (2007). A nasal cannula can be used to treat obstructive sleep apnea. American Journal of Respiratory and Critical Care Medicine, 176(2), 194-200.
Morgan, W. J., Stern, D. A., Sherrill, D. L., Guerra, S., Holberg, C. J., Guilbert, T. W., ...& Martinez, F. D. (2005). Outcome of asthma and wheezing in the first 6 years of life: follow-up through adolescence. American Journal of Respiratory and Critical Care Medicine, 172(10), 1253-1258.
Ordaz, J. M. B., Feixas, T., Calaf, N., González, M., Antón, D., Riu, P. J., &Casan, P. (2009). Ventilatory Pattern monitoring by Electrical Impedance Tomography (EIT) in Chronic Obstructive Pulmonary Disease (COPD) patients. In 4th European Conference of the International Federation for Medical and Biological Engineering (pp. 740-743). Springer, Berlin, Heidelberg.
O'Reilly, N. (2016). History of spirometry. Occupational Health & Wellbeing, 68(11), 21.
Rosengarten, G., Ahmed, B., &Marselli, C. (2003). A novel method to measure respiratory airflow rate based on nasal pressure. IFAC Proceedings Volumes, 36(15), 415-419.
Saboisky, J. P., Gorman, R. B., De Troyer, A., Gandevia, S. C., & Butler, J. E. (2007). Differential activation among five human inspiratory motoneuron pools during tidal breathing. Journal of Applied Physiology, 102(2), 772-780.
Schena, E., Lupi, G., Cecchini, S., &Silvestri, S. (2012). Linearity dependence on oxygen fraction and gas temperature of a novel Fleischpneumotachograph for neonatal ventilation at low flow rates. Measurement, 45(8), 2064-2071.
Shelledy, D. C., & Peters, J. I. (2014). Respiratory care: patient assessment and care plan development. Jones & Bartlett Publishers.
Sierra, G., Telfort, V., Popov, B., Pelletier, M., Despault, P., Lanzo, V., & Agarwal, R. (2006, January). Comparison of respiratory rate estimation based on tracheal sounds versus a capnograph. In 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference (pp. 6145-6148). IEEE.
Snepvangers, Y., de Winter, P., Burger, H., Brouwers, H. A., Bogaard, J. M., & van der Ent, K. (2003). Correction factors for oxygen and flow-rate effects on neonatal Fleisch and Lilly pneumotachometers. Pediatric Critical Care Medicine, 4(2), 227-232.
Usemann, J., Yammine, S., Singer, F., &Latzin, P. (2017). Inert gas washout: background and application in various lung diseases. Swiss Medical Weekly, 147, w14483.
Remember, at the center of any academic work, lies clarity and evidence. Should you need further assistance, do look up to our Engineering Assignment Help
Get It Done! Today
1,212,718Orders
4.9/5Rating
5,063Experts

Highlights
- 21 Step Quality Check
- 2000+ Ph.D Experts
- Live Expert Sessions
- Dedicated App
- Earn while you Learn with us
- Confidentiality Agreement
- Money Back Guarantee
- Customer Feedback
Just Pay for your Assignment
Turnitin Report
$10.00Proofreading and Editing
$9.00Per PageConsultation with Expert
$35.00Per HourLive Session 1-on-1
$40.00Per 30 min.Quality Check
$25.00Total
Free- Let's Start



