- Subject Code : NURBN2012
- University : Federation University My Assignment Services is not sponsored or endorsed by this college or university.
- Subject Name : Medical Sciences
Nursing Practice 3: Pathophysiology and Pharmacology Applied to Nursing
Question 1: Risks that Caused Heart Failure
Heart failure is a chronic and progressive condition where the heart muscle is unable to pump enough blood to meet the blood and oxygen demands of the body (Guazz&Naeije, 2017). The major risk factors that are associated with heart failure in Russel include his medical history of hypertension, cholesterol, alcohol consumption, diabetes, history of chronic smoking, and heart attack (Guazz & Naeije, 2017). Hypertension causes the narrowing of blood vessels and blocks the blood passage. This enhances the chances of developing heart failure. Individuals with a history of smoking are also at a greater risk of developing heart failure. Smoking results in atherosclerosis and contributes toward heart failure. Further, the oxidative stress caused impacts the myocardium leading to systolic and diastolic dysfunction in the individuals. The heart failure in Russel is also associated with his alcohol consumption.
Long term alcohol abuse causes weakening and thinning of the cardiac muscles that affect the ability of the heart to pump blood. As the heart struggles to pump blood efficiently, the lack of blood flow disrupts the major functions of the body resulting in heart failure. Moreover, Russel is also diabetic. Patients with diabetes have an increased risk of developing heart failure. Diabetes causes a reduction in the ejection fraction as excess glucose damages the arteries resulting in atherosclerosis. Russel also has high cholesterol which further contributes to the risk of heart failure by constricting the arteries and restricting the blood flow. Fifteen years back, Russel had also had a heart attack, this can also contribute towards heart failure. Heart attack can lead to heart failure by weakening the pumping ability of the heart. As heart attack causes damage in the cardiac tissue, the muscles fail to contract appropriately hindering the blood supply and weakening the ability of the heart to pump blood.
Question 2: Pathophysiology of The Left Side and Right-Side Heart Failure
Heart failure has been categorized into two types, left side heart failure and right-side heart failure (Zhao & Tian, 2018)
Left-side heart failure
Left-side heart failure occurs when the heart struggles to pump the blood out. Left-sided heart failure occurs when the left ventricle is weak and fails to pump blood appropriately. Left-sided heart failure can be systolic, that is, the left ventricle fails to push enough blood, and diastolic where the ventricle is stiff and fails to relax during ventricular filling (Harjola et al., 2017).
In the case of Russel. Left-sided heart failure is observed with dilatated left ventricle and severe systolic anomaly. In the case of Russel, a dilated left ventricle is observed with an extraction fraction of less than 25%. This condition is called dilated cardiomyopathy and is one of the major causes of heart failure. As the ventricle thins and stretches, it loses its ability to pump blood efficiently and results in heart failure. The major cause of dilated cardiomyopathy has been recognized as hypertension and atherosclerosis, both conditions that have been dominant in Russel. The left-sided heart failure occurs primarily due to anomaly in the cardiomyocyte function, collagen turnover, and changes in the extracellular matrix (Harjola et al., 2017). In the left-sided, systolic heart failure, as the ventricle contracts poorly, there is a decreased volume and pressure and decreased ejection fraction.
This is also associated with anomalies in ATP utilization and electrophysiology of cardiac muscles that occur due to changes in intracellular calcium modulation (Guazz&Naeije, 2017). In left-sided diastolic heart failure, the left ventricular filling is impaired that causes an increase in the left ventricle end, diastolic pressure at rest, or exertion. This occurs as a consequence of an anomaly in the ventricular relaxation, that is an active process. The ventricle may show enlargement and stiffness. CO decreases and the pressure in the pulmonary vein increases. As this pressure exceeds the oncotic pressure of the plasma proteins the fluid is released from the capillaries impacting breathing. This results in lymphatic drainage and causes edema and the ventilation-perfusion is altered. Pleural effusions may develop that can aggravate dyspnea (Francis & Tang, 2019).
Right-Sided heart failure
Right-sided heart failure occurs when the right ventricle fails to pump the blood. The heart failure that involves the right ventricular dysfunction involves a systemic increase in the venous pressure that leads to fluid extravasation and edema. It largely impacts the hepatic and renal function, unlike left-sided heart failure that severely impairs the respiratory system. This also leads to fluid retention in the vital organs (Francis & Tang, 2019). The reduction in the perfusion of skeletal muscles causes atrophy in the cardiac fibres causing weakness, increased fatigue and decreased peak strength. The molecular changes include myocyte hypertrophy, calcium homeostasis regulation anomalies, cross-bridge cycling problems, and changes in the cytoskeletal structures. Changes in the excitation-contraction coupling problems also contribute to heart failure (Francis&Tang,2019).
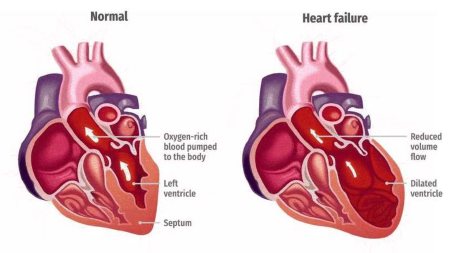
Figure 1: Diagrammatic representation of left ventricular heart failure with enlarged ventricle (Zhao &Tain, 2018)
Question 3: Acute Exacerbation of COPD
Chronic obstructive pulmonary disease (COPD) is a chronic health condition that occurs due to damage in the airways and alveoli (Kim & Lee, 2017). The disease is characterized by the poorly reversible airflow and abnormal inflammatory response in the lungs. The pathophysiology is characterized by mucus hypersecretion and ciliary dysfunction in the respiratory tract. This also causes airflow obstruction and hyperinflation affecting the respiratory cycle of the patient. Systemic inflammation occurs in the skeletal muscles that impact the overall health of an individual suffering from COPD (Kim & Lee, 2017). The exacerbation of the disease is associated with neutrophilic inflammation and an increase in the number of eosinophils. The airway obstruction is increased and pulmonary gas exchange is hindered, this occurs as a consequence of inequality in ventilation and perfusion causing muscle fatigue. This reaction further leads to inflammation, mucus hypersecretion, bronchoconstriction, and edema (Wedzicha et al., 2017). This limits the oxygen availability in the body and triggers hypoxia. Further, respiratory muscle fatigue is also observed in the exacerbation of COPD. This fatigue is responsible for triggering hypoxemia, respiratory acidosis, and hypercapnia directing respiratory failure in the patients (Hikichi et al., 2017).
The major factor that has led to COPD development in Russel is smoking. Inflammation is present in the small airways and lungs of chronic smokers (Anzueto&Miravitlles, 2017). In patients with COPD, the regular inflammatory response against the inhaled toxins is aggravated which further causes tissue destruction, impairment of the defence as well as repair mechanisms in the patients. The inflammatory and the structural changes that are associated with the condition are severe and persist in after smoking cessation in the patients. There is also an anomaly in the proteases and the antiproteases, oxidants, and anti-oxidants in the patients. This results in the development of oxidative stress. As a result of the recognized oxidative stress, the inflammatory response is triggered. Smoke activates the macrophages and the epithelial cells that release chemotactic factors (Hikichi et al., 2017). These chemotactic factors recruit the neutrophils and the CD8 cells from the immune system and cause activation of the fibroblasts (Anzueto&Miravitlles, 2017). As a consequence, an abnormal repair is activates leading to bronchiolar fibrosis and alveolar wall destruction and emphysema. The proteases in the body triggered by smoke or irritant in COPD also causes the release of mucus. This results in an increase in the oxygen burden in the patient further intensifying the reaction in the body (Gelb et al., 2016).
Other factors that are associated with the risk of COPD exacerbation in Russel include occupational exposure to dust and smoke. Russel is a truck driver and therefore, to sustain his work, he is often surrounded by fumes and burning fuel. According to Kim and Lee (2017), occupational exposure to dust, gas, vapour, fumes, etc. are common and significant factors that impact the occurrence and exacerbation of COPD in patients. Since Russel spends a large amount of time on the road, he is at high risk of developing exacerbation of pollutants and fume toxins released by the vehicles.
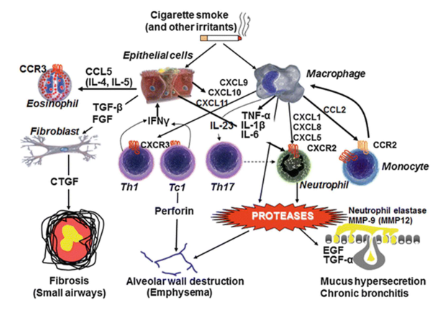
Figure 2: Diagrammatic representation of COPD pathophysiology (Page et al., 2016)
Question 4: Information About Some Drugs Prescribed for Russel
|
Generic name |
Perindopril |
Spironolactone |
Budesonide/ formoterol fumarate dihydrate puffs |
|
Drug group |
Angiotensin-converting enzyme (ACE) inhibitor |
Diuretic. |
Inhaled corticosteroids and long-acting beta2-adrenergic agonists |
|
Mechanism of action |
The somatic ACE has two functional domains at N and C terminus. The active metabolite of the drug competes with ATI for binding to the ACE inhibits causing inactivity of the domain. This prevents the proteolysis and activation of ATI. In turn, this reduces blood pressure (Poulter et al., 2019). |
Competitive inhibitor of mineralocorticoid in the distal convoluted tubule. It inhibits the sodium-potassium exchange channels. This increases the sodium and water excretion from the body. This also enhances retention of potassium (Mleczko-Sanecka, et al., 2017). |
Acts as a bronchodilator. The drug reduces the inflammation of the lungs. Further, formoterol is used to help in the relaxation of muscles in the respiratory tract to ease breathing and prevent spasms (MIMS database, 2019). |
|
Complications or side effects |
Can lead to hypotension, cough, digestive symptoms, fatigue, headaches, and dizziness (Vlachopoulos, & Solomou, 2019) . |
Overuse can lead to drowsiness, mental confusion and nausea in the patients (Mleczko-Sanecka, et al., 2017). |
Common side effects include nervousness and anxiety, chest pain, and trouble in sleeping (MIMS database, 2019). |
|
Nursing considerations |
Monitor the blood pressure of the patient regularly, Serum electrolyte concentration should be carefully monitored, check the patient for allergies by recording accurate medical history (Poulter et al., 2019). |
Record medical history accurately to screen for allergies, monitor the vitals. Monitor the daily I&O and screen for edema (MIMS database, 2019). |
Assessment of medical history for allergies, monitoring of respiratory rate (Kerwin et al., 2018). |
Table 1: Information about some drugs prescribed for Russel.
Question 5: Non-Pharmacological Interventions
Heart failure
- Management of diet, consumption of low-fat, low-salt, and low sugar diet for maintenance of cholesterol levels and sugar levels. A low slat diet will also help in the management of blood pressure (Edelmann et al., 2018).
- Prevent smoking, it is important to avoid smoking to prevent heart failure (Gupta et al., 2016)
- Abstinence of alcohol consumption: This will prevent further damage and atherosclerosis (Thomopoulos&Zanchetti, 2019).
- Increase physical activity and exercise: This will enhance the overall health and prevent cardiac failure (Thomopoulos&Zanchetti, 2019).
Prevention of exacerbation of COPD
- Smoking cessation: Smoking cessation is crucial for people who suffer from COPD to prevent exacerbation. Toxins that are released from smoke and tobacco and further trigger the inflammation reaction and result in breathlessness, airway edema, and mucus secretion in the respiratory tract of the patient (Wedzicha et al., 2017).
- Pulmonary rehabilitation: It uses exercise, education, and behavioural intervention strategies that can assist the patient take necessary steps to avoid exacerbation. It is highly effective for people who suffer from chronic lung disorders like COPD.
Prevention of Pneumonia
- Smoking cessation: Avoid smoking. Pneumonia impacts the lungs and decreases the respiratory capacity of an individual. Therefore, an individual must stop smoking as it can aggravate the inflammatory response, lead to the production of excess mucus in the lungs, cause emphysema, and therefore cause pneumonia in the patients. (Gupta et al., 2016)
- Inclusion of exercise: It is important to do exercise and regularly participate in physical activities. This enhances the overall immunity of the body and also improves the health of organ systems. It, therefore, prevents the occurrence of health conditions like pneumonia and other respiratory problems (Gupta et al., 2016).
- Improvement of diet: The inclusion of a healthy diet that is rich in antioxidants, fibre, and water helps in improving the organ system health and improves cellular immunity. It also assists in combating the damage caused by smoking and pollutants and can, therefore, assist in prevention from pneumonia (Page et al., 2016).
Reduction of cholesterol level
- Intake of a healthy diet: Reduction in consumption of saturated fats, elimination of trans fats, the inclusion of omega 3 rich diets, the inclusion of soluble fibre (Edelmann et al., 2018)
- Physical exercise: Physical exercise can help in losing weight and reduction of cholesterol levels from the body (Edelmann et al., 2018).
- Smoking cessation: Abortion of smoking helps in the reduction of cholesterol levels (Gupta et al., 2016).
References for Pathophysiology and Pharmacology Applied to Nursing
Anzueto, A., &Miravitlles, M. (2017). Pathophysiology of dyspnea in COPD. Postgraduate Medicine, 129(3), 366-374.
Edelmann, F., Knosalla, C., Mörike, K., Muth, C., Prien, P., Störk, S., ... & Group, H. F. D. (2018). Chronic heart failure. DeutschesÄrzteblatt International, 115(8), 124.
Francis, G. S., & Tang, W. W. (2019). Pathophysiology of congestive heart failure. Reviews In Cardiovascular Medicine, 4(S2), 14-20.
Gelb, A. F., Christenson, S. A., & Nadel, J. A. (2016). Understanding the pathophysiology of the asthma–chronic obstructive pulmonary disease overlap syndrome. Current Opinion in Pulmonary Medicine, 22(2), 100-105.
Guazzi, M., &Naeije, R. (2017). Pulmonary hypertension in heart failure: Pathophysiology, pathobiology, and emerging clinical perspectives. Journal of the American College of Cardiology, 69(13), 1718-1734.
Gupta, P., Dewan, P., Shah, D., Sharma, N., Bedi, N., Kaur, I. R., ... & Madhu, S. V. (2016). Vitamin D supplementation for treatment and prevention of pneumonia in under-five children: a randomized double-blind placebo controlled trial. Indian Pediatrics, 53(11), 967-976.
Harjola, V. P., Mullens, W., Banaszewski, M., Bauersachs, J., Brunner‐La Rocca, H. P., Chioncel, O., ... & Fuhrmann, V. (2017). Organ dysfunction, injury and failure in acute heart failure: from pathophysiology to diagnosis and management. A review on behalf of the Acute Heart Failure Committee of the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). European Journal of Heart Failure, 19(7), 821-836.
Hikichi, M., Hashimoto, S., & Gon, Y. (2018). Asthma and COPD overlap pathophysiology of ACO. Allergology International, 67(2), 179-186.
Kerwin, E. M., Siler, T. M., Arora, S., Darken, P., & Rose, E. (2018). Efficacy, safety, and pharmacokinetics of budesonide/formoterol fumarate delivered via metered dose inhaler using innovative co-suspension delivery technology in patients with moderate-to-severe COPD. International Journal of Chronic Obstructive Pulmonary Disease, 13, 1483.
Kim, W. J., & Lee, C. Y. (2017). Environmental exposures and chronic obstructive pulmonary disease. Molecular & Cellular Toxicology, 13(3), 251-255.
MIMS database (2019). Drugs. https://www.mims.co.uk/drugs
Mleczko-Sanecka, K., da Silva, A. R., Call, D., Neves, J., Schmeer, N., Damm, G., ... & Muckenthaler, M. U. (2017). Imatinib and spironolactone suppress hepcidin expression. Haematologica, 102(7), 1173-1184.
Page, C., O’Shaughnessy, B., & Barnes, P. (2016). Pathogenesis of COPD and asthma. In Pharmacology and Therapeutics of Asthma and COPD (pp. 1-21). Springer, Cham.
Poulter, N. R., Dolan, E., Gupta, A. K., O’Brien, E., Whitehouse, A., & Sever, P. S. (2019). Efficacy and safety of incremental dosing of a new single-pill formulation of perindopril and amlodipine in the management of hypertension. American Journal of Cardiovascular Drugs, 19(3), 313-323.
Thomopoulos, C., &Zanchetti, A. (2019). Blood Pressure-Lowering Treatment and the Prevention of Heart Failure: Differences and Similarities of Antihypertensive Drug Classes. In Hypertension and Heart Failure (pp. 285-298). Springer, Cham.
Vlachopoulos, C., & Solomou, E. (2019). Clinical benefits of atorvastatin/perindopril (Euvascor) and atorvastatin/perindopril/amlodipine (Triveram). Medicographia, 41(3), 132-141.
Wedzicha, J. A., Calverley, P. M., Albert, R. K., Anzueto, A., Criner, G. J., Hurst, J. R., ... &Sliwinski, P. (2017). Prevention of COPD exacerbations: A European respiratory society/American thoracic society guideline. European Respiratory Journal, 50(3).
Zhou, B., & Tian, R. (2018). Mitochondrial dysfunction in pathophysiology of heart failure. The Journal of Clinical Investigation, 128(9), 3716-3726.
Remember, at the center of any academic work, lies clarity and evidence. Should you need further assistance, do look up to our Nursing Assignment Help
Get It Done! Today
1,212,718Orders
4.9/5Rating
5,063Experts

Highlights
- 21 Step Quality Check
- 2000+ Ph.D Experts
- Live Expert Sessions
- Dedicated App
- Earn while you Learn with us
- Confidentiality Agreement
- Money Back Guarantee
- Customer Feedback
Just Pay for your Assignment
Turnitin Report
$10.00Proofreading and Editing
$9.00Per PageConsultation with Expert
$35.00Per HourLive Session 1-on-1
$40.00Per 30 min.Quality Check
$25.00Total
Free- Let's Start



